How does an ACL injury occur?
Surgical vs Non-Surgical Management of ACL Ruptures
It is a long held belief in Australia that ACL ruptures must be surgically managed. At this point in time, there isn’t conclusive evidence to suggest that this is the case. Recent research has shown that there isn’t a significant difference between people who underwent ACL reconstruction versus physiotherapy and exercise for their ACL rupture.
This particular piece of research has been ground-breaking for physiotherapists as it provides evidence that ACL injuries can be managed without surgery. Further to this, there are many case studies coming out around the world of people who have had healing of their ACL rupture confirmed on an MRI. The research isn’t at a point where we are able to determine who is likely to have healing and who is unlikely to have this occur but the evidence is strong that it may be possible. The previous thought process was that because the ACL has minimal blood supply, that healing was impossible, evidently this is not the case.
Further strengthening an argument for non-surgical care is that return to sport rates are similar between surgical and non-surgical management. Previous thought patterns were that athletes were unable to return to pivoting sports without an ACL, but there are countless reports of amateur and professional athletes returning to the same level of sport without an ACL.
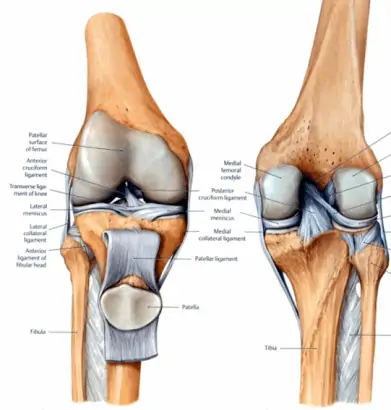
Surgery is the other option, and is performed in approximately 90% of cases of ACL ruptures in Australia. Surgery restores the passive stability of the knee by transferring either a patella tendon graft or hamstring tendon graft in place of where the ACL previously was. The ACL graft is unlikely to be as strong as the native ACL but it provides an increase in support to the knee joint.
Clients are often quoted that ACL reconstruction is likely to reduce the risk of osteoarthritis development, but research has been able to identify that this isn’t the case. It appears as though the cause of the osteoarthritis onset is the ACL injury itself, however in some cases of a meniscus injury being present, surgical management may be recommended.
Other important points to consider for whether you believe ACL reconstruction may be necessary include social and work factors, age (younger clients in their teens may need to wait due to growth plates), your goals for rehabilitation, and other injuries such as meniscus tears or other ligament injuries.
What should physiotherapy/rehabilitation for an ACL involve?
ACL rehabilitation needs to be all encompassing including many different aspects. it is integral that you start physiotherapy and rehabilitation as soon as possible post injury. Early components of physiotherapy are going to include intensive manual therapy and hands on treatment including massage, dry needling, joint mobilisations coupled with a targeted exercise program. As your progress throughout your rehabilitation we will add in components of balance and proprioception, gym strengthening, progress through agility and change of direction skills to build confidence, and eventually progress towards returning to training and returning to sport.
We strongly believe that for optimal recovery after an ACL rupture, field based training should be a part of your physiotherapy regime. We utilise a range of field spaces around North Lakes to conduct this rehabilitation. Without this component of the rehabilitation, returning to training is not optimised. We are able to discuss with you your restrictions because we have already determined what they are and we have seen you do what you will be doing on the pitch or court.
When returning to training, supports such as strapping or braces can be utilised to increase the passive stability of the knee. We don’t want to have to use these in the long term but they can be a great addition to help boost your confidence in the knee when you are working your way back.
With regards to clearance for return to full sport and playing again, an exhaustive testing procedure is completed. It includes clinical tests, a range of questionnaires, physical tests, and fitness and agility tests. We want your knee to be as strong as the other knee, and we want you to be 100% confident in your knee when doing the tests. To ensure we are returning you back to your pre-injury function, we perform these tests on your uninjured knee as soon as possible post injury.
How does PRP Physio structure their ACL Rehabilitation?